Sleeping Pills: What You Need to Know
For some people, sleeping pills can feel like a lifeline when sleep has become difficult. After nights of lying awake, clock-watching, worrying about the next day, or feeling desperate for rest, it is completely understandable to want something that simply helps you switch off.
And sometimes, sleep medication can help. It can provide short-term relief, break an exhausting cycle, or offer support during a particularly difficult period.
But there is an important question beneath the surface: are sleeping pills helping you get natural, restorative sleep – or are they mainly sedating you?
The answer depends on the type of medication, the reason you are not sleeping, how long you take it for, and whether the underlying sleep problem has been properly understood. Not all sleeping pills work in the same way. Some calm the brain, some affect the body clock, and newer medicines target the brain’s wake system. Each has potential benefits, limitations and risks.
In this article, we will look at what sleeping pills actually do, when they may be helpful, when they can cause problems, and what alternatives can help you build better sleep in the long term.
Last reviewed: June 2026
Do sleeping pills give you real sleep — or just sedation?
“Sleeping pills” is a broad term. It can include prescription sleeping tablets, over-the-counter sleep aids, sedating antihistamines, melatonin and newer medicines designed specifically for insomnia.
Most traditional sleeping pills work by calming brain activity so that you feel drowsy and fall asleep more easily. Many work on the brain’s GABA system, which reduces arousal. Others work through histamine, melatonin or orexin pathways.
The key point is this: being sedated is not always the same as having restorative sleep. A medicine may help you get through the night, but that does not automatically mean it has restored the natural rhythm, depth and architecture of healthy sleep.
Some sleeping tablets can affect the quality and structure of sleep. They may help you fall asleep faster or reduce night-time awakenings, but they can also alter the balance of deep sleep and REM sleep, or leave you feeling groggy the next morning.
That does not mean sleeping pills are always “bad”. They can be very helpful as a short-term bridge during difficult periods such as bereavement, acute stress, crisis, travel or severe temporary insomnia.
The issue is not whether medication is good or bad. The real question is: is it the right tool, for the right person, at the right dose, for the right length of time?
Different sleep medications work in different ways. Some mainly sedate the brain. Some help with body-clock timing. Some reduce the brain’s wake signal. Understanding the difference matters.
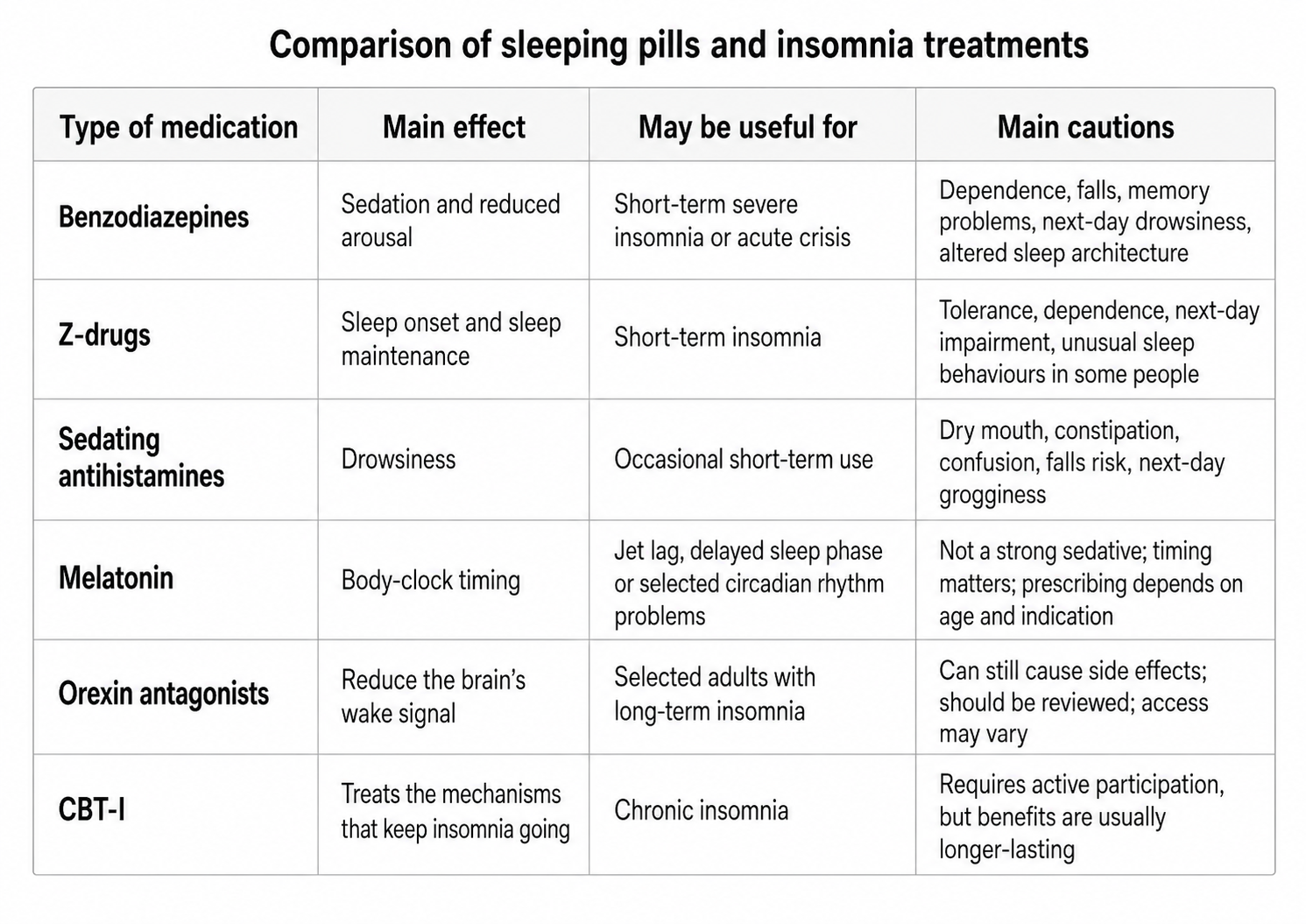
To answer the question properly, we need to separate sleep medication into different groups. Not all sleeping pills work in the same way. Some sedate the brain, some affect the body clock, and newer medicines target the brain’s wake system. That difference matters, because each option has different benefits, risks and limitations.
Do benzodiazepines like lorazepam or temazepam affect sleep quality?
Benzodiazepines, such as lorazepam, temazepam and diazepam, are older medications sometimes used for insomnia or severe anxiety. They can help people fall asleep faster and reduce night-time awakenings.
However, they are sedatives rather than sleep-restoring treatments. They can reduce deep slow-wave sleep, alter REM sleep and cause next-day drowsiness, reduced alertness, impaired coordination and memory problems. They also carry a risk of tolerance and dependence, especially if used regularly or for longer than intended.
In older adults, benzodiazepines can be particularly risky because they increase the risk of confusion, unsteadiness and falls.
What about Z-drugs like zopiclone and zolpidem?
Z-drugs, such as zopiclone and zolpidem, are often prescribed as a more modern alternative to benzodiazepines. They can help with falling asleep and may also reduce waking during the night.
However, they are still usually recommended for short-term use only. Your body can get used to them, their effect can wear off, and dependence can develop if they are taken for longer periods.
Common issues include a metallic taste, dry mouth, daytime sleepiness and next-morning grogginess. Some people also report unusual sleep-related behaviours with zolpidem, such as sleepwalking, making food or making phone calls while not fully awake and not remembering it afterwards.
Alcohol should be avoided with Z-drugs because the combination can increase sedation and make it difficult to wake properly.
Do antidepressants like trazodone or mirtazapine help with sleep?
Some antidepressants are prescribed at low doses because they can have sedating effects. This can be appropriate when insomnia occurs alongside depression, anxiety or another mental health condition.
Mirtazapine
Mirtazapine is an antidepressant that can have a strong sedating effect, especially at lower doses. It can be useful for some people, particularly when poor sleep is happening alongside depression, anxiety, poor appetite or weight loss. In that context, it may help more than one problem at once. However, it is not really a straightforward insomnia medicine, and it is not the first choice if sleep is the only issue. Common side effects include daytime sleepiness, dry mouth, increased appetite and weight gain. Some people also find it leaves them feeling heavy or foggy the next morning, and in some cases it can worsen or trigger restless legs symptoms, which can then make sleep more disrupted.
Trazodone
Trazodone can increase total sleep time for some people and may help with waking during the night. It may be considered when someone has insomnia alongside depression or anxiety, or where sleep maintenance is a particular problem. It can also cause morning grogginess, dizziness, dry mouth and low blood pressure on standing. It is not considered a first-choice treatment for insomnia alone, and the key question is whether it is treating a wider mood or anxiety problem, or simply being used for its sedating side effect.
Amitriptyline
Amitriptyline is another medication people often come across in relation to sleep. It was originally developed as a tricyclic antidepressant, although it is now much more commonly used at lower doses for other problems such as nerve pain, migraine prevention and some chronic pain conditions. Because it can cause drowsiness, it is sometimes prescribed in practice for people who are struggling with sleep, particularly if pain is also part of the picture. However, it is not a first-line treatment for insomnia and should not be thought of as a simple sleeping tablet. Side effects can be significant and include dry mouth, constipation, dizziness, falls and next-day grogginess. It also needs extra caution in older adults or people with certain heart conditions.
With, the decision depends on the bigger clinical picture, not just whether the medicine makes you sleepy. These medicines can be very helpful in the right clinical context, but they should not be seen as simple sleeping tablets. The underlying diagnosis matters.
Do over-the-counter antihistamines work as sleeping pills?
Many over-the-counter sleep aids contain sedating antihistamines such as diphenhydramine. These can make you feel drowsy and may help you fall asleep in the short term.
However, they can also cause dry mouth, constipation, urinary problems, blurred vision, next-day grogginess and confusion. They can be especially problematic in older adults, where they may increase the risk of falls or delirium.
Over-the-counter does not always mean low-risk. It is still worth checking with a pharmacist or GP, especially if you take other medication, drink alcohol, are pregnant or breastfeeding, or are over 65.
What are orexin antagonists, and are they better for sleep?
Newer insomnia medicines called orexin antagonists work differently from traditional sleeping tablets. Instead of broadly sedating the brain, they reduce the brain’s wake-promoting signal.
Daridorexant is a dual orexin receptor antagonist licensed for insomnia. NICE recommends daridorexant for some adults with long-term insomnia, where symptoms occur at least three nights per week for at least three months, daytime functioning is affected, and CBT-I has not worked, is unavailable or is unsuitable.
This is an important development in insomnia treatment because it offers a different mechanism from older sedative medications. It has less impact on the natural balance of sleep stages than traditional sleeping tablets and has been shown to improve how people feel during the day, as well as how they sleep at night.
However, it is not a magic bullet, and it is not side-effect free. Possible side effects include headache, dizziness, fatigue, nausea, sleepiness and, less commonly, sleep paralysis or hallucinations. Treatment should be reviewed, and if it is not helping enough, it should be stopped in discussion with the prescribing clinician.
Does melatonin improve sleep quality?
Melatonin is a hormone involved in regulating the body clock. It is often misunderstood as a natural sleeping pill, but it is better thought of as a circadian timing signal.
Melatonin is usually most helpful when the problem is sleep timing rather than simply sleepiness. This may include jet lag, delayed sleep phase, some neurodevelopmental conditions, or other circadian rhythm problems.
It does not act like a strong sedative. Taking more is not necessarily better, and timing matters greatly. If it is taken at the wrong time, it may be ineffective or may shift the body clock in the wrong direction altogether.
In the UK, melatonin prescribing depends on age, formulation and indication. It may be prescribed short-term for some adults over 55, for jet lag in certain situations, or under specialist guidance in younger adults and children.
What is causing the poor sleep?
So far, we have looked at what different sleep medicines can do. But the bigger question is often this: why is sleep difficult in the first place?
One of the most important things to understand is that poor sleep is not always insomnia.
A sleeping tablet may reduce wakefulness temporarily, but it will not treat the underlying cause if the real issue is:
- obstructive sleep apnoea
- restless legs syndrome
- pain
- night sweats or menopause symptoms
- anxiety, depression, trauma or burnout
- alcohol use
- stimulant medication
- nocturia
- shift work
- jet lag
- an irregular body clock
- not having enough opportunity to sleep
Before reaching for medication, it is worth asking: what is actually driving the sleep problem?
If you have undiagnosed obstructive sleep apnoea, some sleeping pills can make the situation worse. They may relax airway muscles, increase sedation, reduce your ability to wake in response to breathing pauses, or worsen next-day sleepiness.
Speak to your GP before taking any sleeping tablets if you:
- snore loudly
- stop breathing during sleep
- wake gasping or choking
- wake with morning headaches
- feel very sleepy in the day despite spending enough time in bed
- have high blood pressure or atrial fibrillation alongside poor sleep
Treating sleep apnoea can transform sleep quality, energy, mood and long-term health. In this situation, sleeping tablets are not the solution to the real problem.
Are sleeping tablets addictive?
Yes, some prescription sleeping tablets can lead to tolerance and dependence, particularly benzodiazepines and Z-drugs.
Tolerance means your body gets used to the medication, so the same dose no longer has the same effect. Dependence means your body has adapted to the medication, and stopping it suddenly can cause withdrawal symptoms or rebound insomnia.
Rebound insomnia can feel frightening. Sleep may temporarily become worse when a sleeping tablet is reduced or stopped, even if the original sleep problem has improved. This is one reason why people can feel trapped on sleep medication for longer than they intended.
If you are already taking sleeping tablets regularly, do not stop suddenly without medical advice. Many people need a gradual reduction plan alongside behavioural support for insomnia.
Who should be especially cautious with sleeping tablets?
Sleeping medication needs extra care if you:
- are over 65
- snore loudly or may have sleep apnoea
- drink alcohol in the evening
- take opioids, strong painkillers, sedatives or other medicines that make you drowsy
- are pregnant, breastfeeding or trying to conceive
- have liver or kidney problems
- have a history of falls, confusion or memory problems
- have a history of drug or alcohol dependence
- have severe depression, suicidal thoughts or significant mental health concerns
- need to drive, operate machinery or make safety-critical decisions the next morning
In these situations, a medication review and proper sleep assessment are particularly important.
The best alternative depends on the cause of the sleep problem. For chronic insomnia, the most effective long-term approach is usually Cognitive Behavioural Therapy for Insomnia, known as CBT-I.
What is CBT-I?
CBT-I is the "gold standard" treatment for chronic insomnia. Unlike sleeping tablets, it does not simply make you drowsy. It treats the patterns that keep insomnia going.
It is an evidence-based therapy that helps people break the cycle of sleeplessness by addressing both the cognitive (thought-based) and behavioural aspects of insomnia. This approach targets two main areas: the unhelpful thoughts that keep you awake at night and the behaviours that make it harder to fall asleep or stay asleep.
The process typically takes four to six sessions, either with a therapist or through an online programme, where individuals learn techniques to restructure their thinking and habits. CBT-I helps people develop healthier sleep patterns by focusing on actions such as:
-
Adopting better sleep habits: This includes practices like avoiding stimulating activities before bed, creating a comfortable sleep environment, and sticking to a consistent sleep schedule. The goal is to prime both the mind and body for restful, uninterrupted sleep.
-
Behavioural interventions: CBT-I gives you a toolbox of techniques you can use to prime your body for sleep, meaning you get to sleep and stay asleep through the night.
- Changing thoughts about sleep: Many people with insomnia become anxious or stressed about not being able to sleep, which ironically makes it harder to rest. CBT-I teaches individuals how to reframe these thoughts, replacing them with more positive and realistic expectations.
Research consistently shows that CBT-I is highly effective for people with chronic insomnia. In fact, between 70% and 80% of individuals who try CBT-I report significant improvements in their sleep patterns. Unlike medications, the benefits of CBT-I are long-lasting, with many people continuing to see improvements even a year after completing therapy.
It does not matter what the underlying cause for your insomnia is: whether it's mental health concerns, menopause symptoms or chronic pain, the evidence shows CBT-I works just as well at improving sleep and health outcomes.
Is sleep hygiene enough?
Sleep hygiene can be useful, but it is usually not enough on its own for chronic insomnia.
Foundations such as regular wake times, morning daylight, limiting caffeine later in the day, keeping the bedroom cool and reducing alcohol can all support healthy sleep. But if you have had insomnia for months or years, you usually need more than general tips.
This is where CBT-I is different. It is not just “avoid screens and have a bath”. It is a structured treatment that targets the behavioural and psychological cycle of insomnia.
Medication can be a bridge, not the destination
Sleep medication can sometimes provide a bridge through a difficult patch. For example, it may help someone cope during acute grief, severe temporary stress, travel disruption or a crisis.
But for ongoing insomnia, the long-term goal is usually to rebuild confidence in sleep, restore rhythm, and treat the reason sleep has become difficult in the first place.
If you are considering sleeping medication, or you are already taking it, these questions can help guide the conversation:
- What type of sleeping tablet is this?
- Is it intended for short-term or longer-term use?
- How long should I take it for?
- What is the plan for stopping it?
- Could I have sleep apnoea, restless legs, menopause-related sleep disruption or another underlying cause?
- Could any other medications I'm taking be affecting my sleep?
- Is it safe with alcohol or my other medicines?
- Will it affect driving or work the next morning?
- Would CBT-I be more appropriate?
You should seek professional support if:
- insomnia lasts more than a few weeks
- poor sleep is affecting your mood, concentration, work or relationships
- you feel sleepy in the day despite spending enough time in bed
- you snore loudly, stop breathing, wake gasping or have morning headaches
- sleep problems are linked with low mood, anxiety, trauma or burnout
- you are relying on alcohol, antihistamines or sleeping tablets to get through the night
- you have been taking sleeping tablets for longer than planned
Sleep problems are common, but they are not something you simply have to live with. The right treatment depends on the right diagnosis.
Here are some of the most common questions people ask when they are considering sleeping tablets:
Do sleeping pills give you proper sleep?
Sometimes they help, but they do not usually produce the same quality of sleep as natural sleep. Some sleeping tablets increase the time you are asleep, but change the pattern and quality of sleep or cause next-day grogginess.
Are sleeping pills bad for you?
Not always. Sleeping pills can be useful in selected short-term situations. The risks increase when they are used regularly, for too long, at higher doses, with alcohol, or without addressing the underlying cause of the sleep problem.
How long can you take sleeping tablets for?
Many traditional sleeping tablets, such as Z-drugs, are usually prescribed for short-term use only. The exact duration depends on the medication and your individual circumstances, so always follow the advice of your prescriber.
Can sleeping tablets make sleep apnoea worse?
Yes, some sedative medications can worsen sleep apnoea or increase the risk of breathing-related problems during sleep. If you snore loudly, stop breathing, wake gasping or feel very sleepy in the day, speak to your GP before taking sleeping tablets.
Is melatonin a sleeping pill?
Melatonin is not a sleeping pill in the traditional sense. It is a hormone involved in body-clock timing. It can help with selected circadian rhythm problems, but it is not a strong sedative, and it does not work for everyone.
What is the best alternative to sleeping pills?
For chronic insomnia, the best-supported alternative is CBT-I, or Cognitive Behavioural Therapy for Insomnia. It treats the thoughts, behaviours and body-clock patterns that keep insomnia going.
Sleeping pills can be a helpful bridge during short-term sleep struggles, but they are not the long-term answer for most people with chronic insomnia.
They may increase the number of hours you sleep, but that does not always mean they restore natural, refreshing sleep. They can also cause grogginess, tolerance, dependence, falls, interactions with alcohol or other medication, and problems if the underlying issue is sleep apnoea or another untreated sleep disorder.
The most effective approach is to understand what is causing the sleep problem and choose the right treatment. For chronic insomnia, CBT-I remains the first-line option because it helps rebuild your ability to sleep without relying on nightly medication.
At The Sleep Project, we help people move beyond quick fixes and build a more sustainable relationship with sleep. Our Retrain Your Sleep CBT-I programme is designed to help you understand your sleep, reduce insomnia patterns and build lasting, restorative sleep.
This article is educational and does not replace medical advice. Medication decisions should always be made with a qualified healthcare professional who knows your medical history.
Declaration of interest: Dr Eidn Mahmoudzadeh has previously received payment from Idorsia Pharmaceuticals for delivering educational sessions on insomnia to healthcare professionals. Idorsia has had no involvement in the writing, review or approval of this article and has no involvement in The Sleep Project’s clinical recommendations, services or business activities.
References
- NICE Technology Appraisal TA922: Daridorexant for treating long-term insomnia
- NICE Clinical Knowledge Summary: Insomnia
- NHS: About zopiclone
- NHS: Common questions about zopiclone
- NHS: Common questions about zolpidem
- NHS: Common questions about melatonin
- NHS: Sleep apnoea
- NHS: Diphenhydramine
- BNF: Daridorexant
Join our mailing list below to get exclusive early access to
free educational content, tools and other goodies!
We won't send spam. Unsubscribe any time.